- They can be armed with beta or alpha warheads
- Deposit radiation dose systemically to treat advanced disease
- Can be imaged to diagnose disease select and track patients
- Imaging inform distribution and dosimetry
Development is complex:
- Added complexity to the discovery process
- Requires multidiscriplinary expertise in several areas – biochemistry, radiochemistry, imaging and medical physics
- Also logistics due to half life and manufacturing can be more complex.
Usually are highly cancer specific, high persistent expression throughout the tumor and metastasis, readily accessible on the cell surface, not shed and thoroughly validated.
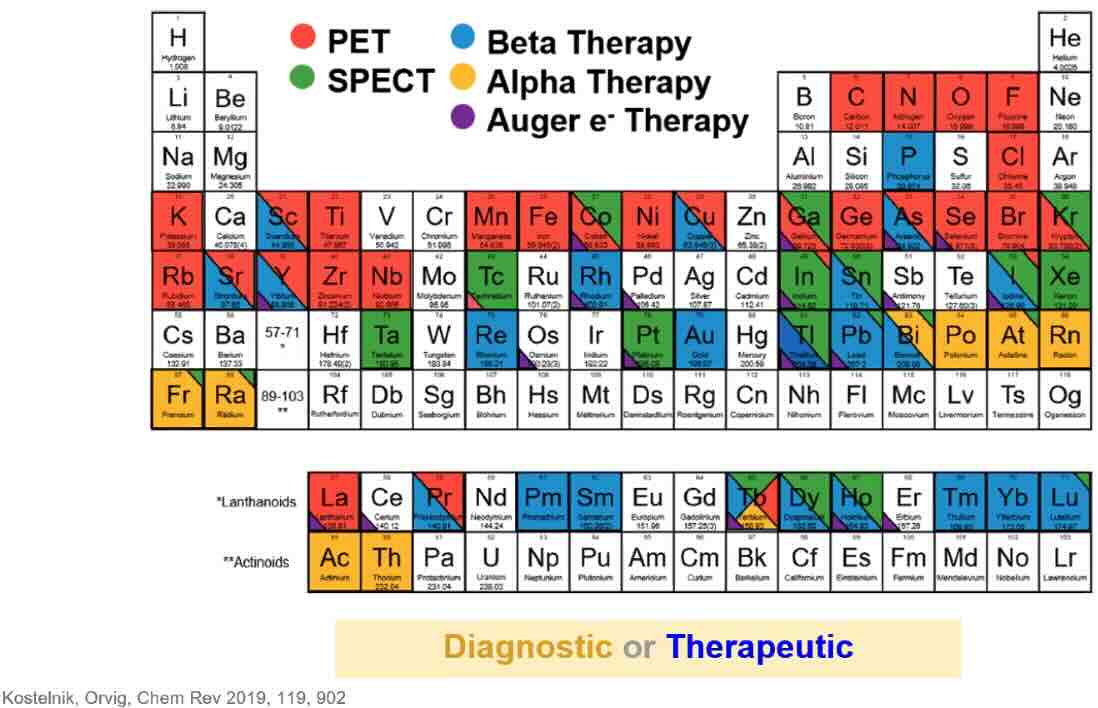
Many isotopes are possible and many targets possible such as Nectin4, DLL3, FAP, Somatostatin receptors, PSMA, Integrins, CXCR4, Claudin 18.2, Norepinephrine transporter, EGFR2.
Clearance from tumor will matter on its effectiveness – if cleared rapidly then it will not have time to act. If internalized, then there may be an effect – for example covalent binders may increase activity. Internalization is important for efficacy rather than safety – and plays into the therapeutic window.
The radioactive entity is the active moiety and that drives the pharmaceutical property. Toxicity profile is determined by how they are distributed through the body.
Note : Albumin binding can enhance the half life whereas salivary gland or delayed renal toxicity can be limiting to effectivity.
There are 2 approved recently: Lutathera and Pluvicto and both are owned by Novartis. They both use the Lutetium -177 isotope.
- Lutathera – Targets the somastatin receptor subtype 2 (SSTR2) for diagnostic companion, approved in 2018
- Pluvicto – Prostrate specific antigen. (PSMA)
Pioneers have been Bayer and Novartis have been those that have acquired rights, but others have been active too: BMS, Lilly, AZ, Lantheus which are mostly Actinium -225 based drugs.
Actinium-225 demand because of alpha-emitting isotopes for highly targeted potent cancer killing.
Future is distributed manufacturing network not necessarily new molecules.
Beta emitters (Lu-177) have been used first but Ac-225, At-211 and PB-225 are becoming more prevalent.
Alpha emitters are longer lived, have higher potency, and need minimal shielding though alpha emitters is more complex. Alpha agents can increase potency but more difficult to source, redcued shelf life, daughter relocation and introduciwng potential normal tissue toxicitiy.
Ritumximab made the jump from lymphoma to rheumatoid arthiritis.
Comparison of RLT to other ADC makes them comparable though hard to do cross trial comparisons.
CAR-T though achieves functional cures.
What is not in guidance for industry for Radiopharmaceuticals:
- Mass dose optimization is not stated
- Model informed drug development to support dose optimization (it is present in general drug development guidance though)
- Subpopulation
- Theranostics approach for patient selection and dose optimization